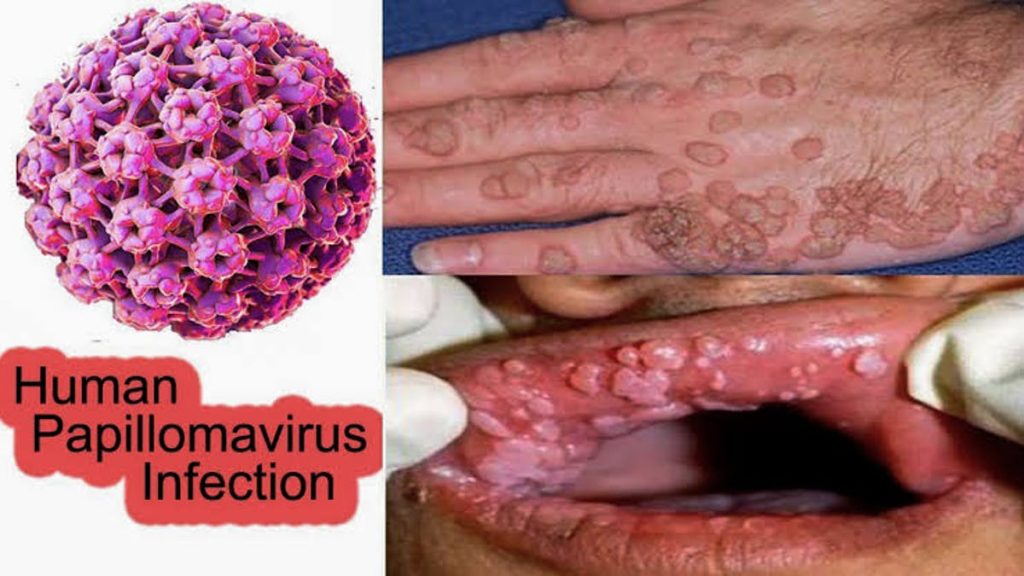
Human papillomavirus infection (HPV) is currently the most prevalent sexually transmitted disease (STD) in the world. This infection is caused by more than 150 types of virus and its main symptoms are the appearance of warts on the hands, feet and genitals, where they are also known as condyloma acuminata.
HPV was first described in 1935 by Dr Francis Peyton Rous, who had demonstrated the existence of a virus with oncogenic (capable of inducing the formation of tumors) that caused cancer in the skin of rabbits and whose description coincided with the papillomavirus.
High or low risk virus terms are used to classify the various papillomavirus serotypes according to their greater or lesser capacity to cause malignant transformation of the cells they infect, degenerating into a neoplasm or cancer.
The transforming activity of the virus is due to the action of two constitutive proteins called E6 and E7 oncoproteins which interact with a large variety of receptors involved in various biological processes. Such as, programmed cell death or apoptosis, division, proliferation and differentiation cellular.
Serotypes of high-risk human papillomavirus include 16 and 18, which cause approximately 70% of cervical cancers. Other high-risk viruses are 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73 and 82.
The serotypes considered to be of low risk are hpv 6 and 11, which cause about 90% of genital warts which rarely turn into cancer. Genital warts can seem raised bumps or growths that sometimes are cauliflower-shaped and can appear weeks or months after exposure to a sexual partner infected.
The human papillomavirus belongs to a family of viruses called Papillomaviridae whose only genus is the papillomavirus: These are double-stranded acid (DNA) viruses that preferentially infect skin cells and mucosal epithelia (genitalia, anus, mouth, or respiratory tract).
100 types of hpv are known, about sixty types produce warts on areas such as the hands or feet and are transmitted person to person by direct contact with these lesions. The other types of viruses about forty serotypes are transmitted sexually and present affinity for the mucous membranes of the body, such as layers of wet around the anal and genital.
In summary, the papillomavirus infection can be transmitted by contact with the skin of external infected genitalia, the mucous membranes or body fluids,through sexual intercourse and oral sex.
Factors that increase the risk of becoming infected with a sexually transmitted disease such as papillomavirus include:
HPV doesn’t manifest symptoms in many people and doesn’t lead to health problems. However, when HPV infection is not cured and depending on the type of virus involved (as explained in the previous section), it can result from genital warts to serious diseases, like various cancers. The following describes the symptoms and the evolution of these pathologies in both sexes.
In women, the papillomavirus can cause the appearance of genital warts, which can be of various sizes – flat or elevated. If you do not follow any treatment, over time these warts can disappear, remain unchanged or grow and multiply.
The evolution of cervical cancer involves the progressive development of several stages. First the cervical epithelial cells have certain histological abnormalities known as cervical intraepithelial neoplasia (CIN) or mild dysplasia; then occurs the moderate dysplasia; in the third place, occurs severe dysplasia or carcinoma in situ and finally, invasive cancer.
Several epidemiological studies have shown that approximately 85% of severe dysplasias have papillomavirus DNA and 100% of invasive cervical cancers have the virus.
The papillomavirus is infecting cells or tissues, which are still apparently normal and the patient lacks clinical manifestations; Yet the virus is present and can only be detected by molecular biology techniques such as polymerase chain reaction (PCR).
The papillomavirus has caused small microscopic changes in the epithelial cells of the cervix: This is known as coilocytic changes or dysplasia, which can be evidenced in routine cytology or in a biopsy of the affected tissue. At this stage of the infection the presence of the virus can also be detected macroscopically in a routine gynecological examination by the use of a solution with iodine or acetic acid; If coloration changes are observed, the presence of a premalignant lesion is highly probable.
Characterized by the presence of malignant tumors; The virus is capable of multiplying rapidly and may cause infection of other neighboring tissues.
Cancer of the vulva is a rare entity which constitutes 4% of gynecological cancer. It is characterized by the formation of tumor cells in the tissues of the vulva, usually in the labia majora. Papillomavirus infection and advanced age increase the risk of this disease.
Signs and symptoms of vulvar cancer include a nodüle,ulcer lesion, pruritus,stinging, irritation, bleeding and hypersensitivity in the vulvar area: it may be most characteristic symptoms of infections of the lower urinary, such as dysuria.
The main histological type of cancer of the vagina that is related to the persistent infection by human papillomavirus is the squamous cell carcinoma; it has been reported that the virus is responsible for 70% of the cases. This type of cancer is more frequent in women american, black and older than 60 years.
At the beginning of the disease, patients are asymptomatic, but as it progresses, there is usually an intermenstrual vaginal bleeding, especially after intercourse. The most frequent symptom of patients with cancer of the vagina is bleeding which may occur after intercourse, before puberty or after menopause.
Most men who are infected with the papilloma virus show no symptoms. HPV can also cause genital warts in men, as well as in women. Warts can be single or multiple and have various forms: Cauliflower, raised or flat and usually appear around the anus, on the penis, on the skin (covering the testicles), the groin region, the glutes or on the thighs. The lesions can appear in a time that goes from weeks to months after the sexual contact with the person infected.
It is important for men to understand how to reduce the risk of infection with this virüs, as it may increase the risk of genital cancer, although this is not the most common.
About thirty serotypes of papillomaviruses are associated with anal cancer and penile cancer have been reported in the literature, although they are rare pathologies in immunocompetent men. The American Cancer Society estimates that by 2012 about 1,570 men in the United States will be diagnosed with penile cancer and about 2,250 men could be diagnosed with anal cancer. The risk of anal cancer is approximately 17 times higher in sexually active as homosexual and bisexual men than in men who have sex with only women. Likewise, men with human immunodeficiency virus (HIV) infection are also at higher risk for this type of cancer.
It is estimated that about 7% of adults in the United States have oral papillomavirus infection, with the most common serotype HPV 16. The same type that produces a significant percentage of cervical cancer. Recent studies predict that by 2020 there will be more cases of men with oral cancer in relation to papillomavirus infection than cases of women with cervical cancer.
A few years ago tobacco and alcohol were thought to be the main cause of most cases of oropharyngeal cancer (a type of cancer in the mouth, which mainly affects the base of the tongue and the back of the tongue).
In an effort to better understand the role of oral papillomavirus infection and how it affects the risk of head and neck cancer, US investigator Dr. Gillison and his group analyzed mouthwash samples from a group of people aged between the ages of 14 and 69 during the period in 2009-2010.
Among the main findings, 10.1% of men and 3.6% of women had evidence of oral papillomavirus infection;
The diagnosis of HPV infection (human papillomavirus) is performed with the following tests:
This includes the direct observation of the genital warts. Acetic acid can be used which stains white lesions. It is also observed by colposcopy of the cervix and vagina previously stained with iodine or acetic acid.
Observation of suspicious cells with coilocytic changes in cytology of the cervix and vagina in women, using the Papanicolaou stain. Biopsies may be taken of suspicious lesions, neoplasm or genital warts in both men and women. These samples are sent to a section of pathological anatomy for analysis.
Direct detection of the genetic material of the virus by techniques of molecular biology:This amplifies the DNA of the virus and allow the identification of the different serotypes.
Treatment of HPV (human papillomavirus) infection can vary depending on a number of factors including type of lesion (warts, precancerous or cancerous lesions), anatomical location of lesions and number of lesions.
The treatment of HPV-originated warts includes:
Topical application of podophyllin 0.5% directly on the wart which can be applied by the same patient twice a day for three consecutive days.
Topical application of Imiquimod to 5% (Aldara in cream). This immunomodulatory drug acts by activating the cells of the immune system that attack and destroy the virus. Imiquimod can be applied by the same patient, once a day before bed, three times a week, for a maximum period of 16 weeks. After six to ten hours of action, the medication must be removed from the area with plenty of soap and water. This treatment isn’t suitable in pregnancy. It may present slight redness of the area and pruritus.
Application of 80-90% trichloroacetic acid: This substance is a very strong acid that should only be applied topically with an applicator in the area of the lesion by a specialist doctor.
Other ways of removing warts that should be performed by medical specialists are cryotherapy with liquid nitrogen, surgical removal by electrocoagulation or by the use of laser.
If a woman with a precancerous lesion by human papillomavirus receives the right treatment in time she has a high rate of healing and survival. The therapeutic approach of these lesions consists of:
The tissue is frozen using a metal probe that has been cooled with nitrous oxide or carbon dioxide circulating inside the probe. It has an effectiveness ranging from 85 to 95% and is only used in the case of small lesions of approximately 20 millimeters or less and do not extend within the canal of the cervix.
Involves removal of the affected area with a hot handle like the scalpel, and requires the use of local anesthesia. It has a 95% effectiveness for the removal of the injury.
It consists in removing the affected tissue with the shape of a cone of the cervix using a scalpel. Although no longer the treatment of choice for pre-cancerous lesions, can still be used in cases of injuries that can be treated in another way or when cancer is suspected. It has an effectiveness of 94%, requires the use of anesthesia and has as its main complication is bleeding in the area, as well as the risk of stenosis (narrowing) of the canal of the cervix.
If a person has been diagnosed with any type of cancer associated with papillomavirus infection, the behavior of the specialist doctors will depend on the location of the lesion and the extent of the neoplasia. Treatment may include surgical procedures, chemotherapy and radiation therapy.
Microimmunotherapy is little known among physicians however it has been applied in the world for about 35 years with good results. It was born in 1967 when Dr. Maurice Jenaer discovered that when Nucleic Acids (DNA and RNA) were administered in highly diluted proportions to cancer patients that they were able to stimulate their immune system and the patient improved. Since then, several researches and studies have made possible the development of a therapeutic system that is used in the effective treatment of any disease.
To prevent infection by the HPV (human papilloma virus), in addition to limit risk factors, such as avoiding promiscuity and unprotected sex, experts recommend administration of the HPV vaccine.
The first vaccine developed and marketed to prevent cervical cancer, precancerous genital lesions and warts due to papillomavirus.It has been available since 2006 under the name Gardasil, which consists of an injectable suspension of the purified L1 proteins of four Virus serotypes: 6, 11, 16 and 18.
Gardasil is administered to female patients (aged 9 to 26 years) in three doses, allowing two months to pass between the first and second doses and four months between the second and third doses. The vaccine is given as an intramuscular injection (injection into a muscle), preferably into the arm or thigh.
The second vaccine has been available since 2009 and is called Cervarix. It contains a suspension of the major antigenic protein that comes from the capsid of oncogenic types 16 and 18, this is the L1 protein. Cervarix is a vaccine which is for the prevention of diseases caused by oncogenic viruses 16 and 18: Cervical cancer, cervical intraepithelial neoplasia (NIC) 1 and 2, as well as adenocarcinoma in situ. Its use is approved in women aged 9 to 26 years. Immunization with Cervarix is done by the application of three doses of the vaccine intramuscularly in the deltoid region of the arm at 0, 1, and 6 months.
In 2011, The US Vaccine Committee and the Atlanta Center for Infectious Diseases (CDC-Atlanta) recommended Gardasil vaccine against papillomavirus in male patients aged 11 to 21, with the age of vaccination extended to The 26 years in the case of homosexuals and men with the depressed immune system.
In December 2014, the World Health Organization (WHO) presented the new version of the Comprehensive Guide to Cervical Cancer – A Guide to Essential Practices which recommends giving girls between the ages of 9 and 13 two doses of the vaccine compared to the papillomavirus. Because, this vaccination schedule is just as effective as the one of three that was carried out to date and facilitates the administration of the vaccine and reduces its cost.
Medical Referral | Accident Attorney Referrals
Filter out the noise and nurture your inbox with health and wellness advice that’s inclusive and rooted in medical expertise.
MedicalReferral.com does not provide medical advice, diagnosis, or treatment.